Introduction
The major artery carrying blood from the heart is called the Aorta. Branches from this supply blood to the body. In the abdomen the aorta has branches to the liver, spleen, gut and kidneys and then divides into the leg arteries. This last part of the aorta before it divides can become dilated and is called an aneurysm.
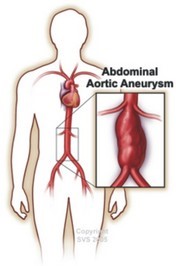 This occurs most often in men aged 60 and over. Aneurysms are more common in people who smoke and have high blood pressure. There can be a family history of the condition. As the dilatation progresses (like a worn out bicycle tyre or inner tube) the wall of the aorta is stretched and becomes thinner. This can lead to the wall tearing leading to internal bleeding. This is called Aneurysm Rupture. Sometimes clot forms within the aneurysm and this can cause problems with the circulation to the legs.
This occurs most often in men aged 60 and over. Aneurysms are more common in people who smoke and have high blood pressure. There can be a family history of the condition. As the dilatation progresses (like a worn out bicycle tyre or inner tube) the wall of the aorta is stretched and becomes thinner. This can lead to the wall tearing leading to internal bleeding. This is called Aneurysm Rupture. Sometimes clot forms within the aneurysm and this can cause problems with the circulation to the legs.
How do I know if I have an Aneurysm ?
The majority of AAA's cause no symptoms and are discovered by chance. An examination by your GP or a scan performed for another reason may pick up the AAA. Some patients are aware of a prominent pulsation in the abdomen. Rarely the AAA may cause some back pain and abdominal pain. Since AAA does not cause symptoms it makes sense to screen for the condition. There is now a national screening programme for AAA.
What is the chance of an AAA rupturing?
The chance of rupture is very low for small AAAs. For aneurysms measuring less than 5.5cm in diameter the risk of rupture is less than 1 in 100 per year. As aneurysms get larger than 5.5cm, the risk of rupture increases and it is usually at this size that the option of surgery is considered. For any given size, rupture risk is increased in smokers, those with high blood pressure, and those with a family history of an AAA.
Each individuals risk from their AAA and from surgery may be different so any decision on treatment will be carefully considered by your vascular team and always discussed in detail with you and, when appropriate, your family.
Should everyone with an AAA have surgery?
The short answer is no. Surgical repair of an AAA is a major operation and carries risks. Research has shown that for people with aneurysms, measuring less than 5.5cms (about 2 inches), it is safer not to operate as the risks of having an operation are greater than the benefit
Surveillance of small AAAs
If your aneurysm is smaller than the size at which operation is needed, your surgeon will arrange further ultrasound scans (usually every 6 to 12 months) to monitor the rate of growth. Most aneurysms grow slowly at a rate of about 3mm (1/8th inch) per year but larger aneurysms can grow more quickly. How often you will need to have a scan will depend on the size of your aneurysm. Your blood pressure will be checked and you will be given advice about managing your risk factors and staying healthy.
If you have any worries or concerns about your aneurysm you can discuss them with your vascular surgeon or nurse. If your aneurysm starts to produce symptoms, or rapidly increases in size (as measured by the scan), you will be seen by your vascular surgeon who may recommend an operation to repair it. If you need treatment for your aneurysm you will be given more information.
Treatment Options for AAAs
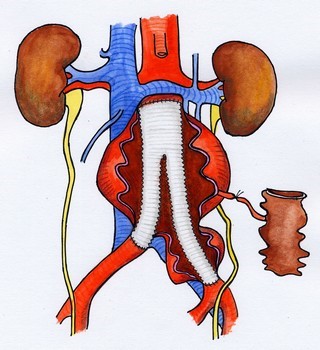
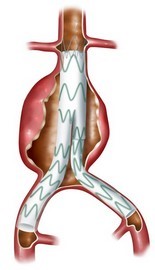
Surgery is commonly advised if you develop an AAA larger than 5.5cm in maximum diameter (about 5 cm in women). For these larger aneurysms the risk of rupture is usually higher than the risk of surgery. If you have a family history of ruptured aneurysm; surgery is also likely to be advised. The two types of operation available to repair your AAA are Open Surgery or Endovascular Repair.
 However, if your general state of health is poor, or if you have certain other medical conditions, this may increase the risk if you have surgery. In some circumstances therefore the decision to operate may not be straightforward, and your surgeon may advise that you be medically managed if you are unfit for surgery.
However, if your general state of health is poor, or if you have certain other medical conditions, this may increase the risk if you have surgery. In some circumstances therefore the decision to operate may not be straightforward, and your surgeon may advise that you be medically managed if you are unfit for surgery.
If you are being considered for treatment you will undergo tests of your fitness for surgery and the associated risks , along with a CT scan to examine your AAA more closely. Your specialist vascular surgeon and team will give you a clear explanation of the options in your case. You will then have full discussion involving your personal choice before a decision is made. Your best interests will always be taken into account and you are not obliged to undergo any treatment that you do not want.
Medical Treatment
If you are unfit for surgery at the current time, your doctor may wish to advise medical treatments aimed at keeping you healthy and reducing the risks of rupture of your AAA. These will include treating any high blood pressure and high cholesterol and improving your fitness by treating any heart lung or kidney disease so that an operation may be performed at a later time. Patients with diabetes are less likely to have problems with surgery if their diabetic control is good. Regular moderate exercise can also help keep your heart and lungs healthy.
For further information click HERE